
Pain Reprocessing Therapy in Seattle, WA
If you’ve tried medical treatments, physical therapy, or multiple approaches, and your pain still isn’t improving —
there may be a different explanation.
I offer in-person therapy in Seattle, WA and virtually throughout Washington, Oregon and Utah

Chronic Pain Therapy in Seattle
I provide chronic pain therapy in-person in Seattle, WA for individuals experiencing persistent pain that hasn’t responded to traditional medical or physical treatments. My work is grounded in modern pain science and focuses on how the nervous system learns and maintains pain over time.
Rather than treating pain as purely structural, this approach looks at the neurological and emotional patterns that keep pain active—helping you understand what’s happening in your body and begin to shift it.
When Doing Everything Right Still Hasn’t Helped
Living with chronic pain often means living with uncertainty — about your body, your future, and whether anyone truly understands what you’re experiencing.
Most people who end up here have already tried to figure it out.
They’ve done the appointments, the treatments, the research—only to be left with symptoms that don’t follow a clear pattern or explanation.
At a certain point, it’s not about trying harder…
…It’s about understanding what’s actually keeping the pain going.

What If There Was Another Way?
Pain is not a direct measure of damage in the body. It is a protective signal created by the nervous system to keep you safe.
When the brain perceives something as a threat, it can produce pain—even when there is no ongoing injury. Over time, this can become a learned pattern.
This is what often happens in chronic pain: the system learns a pattern that keeps repeating.
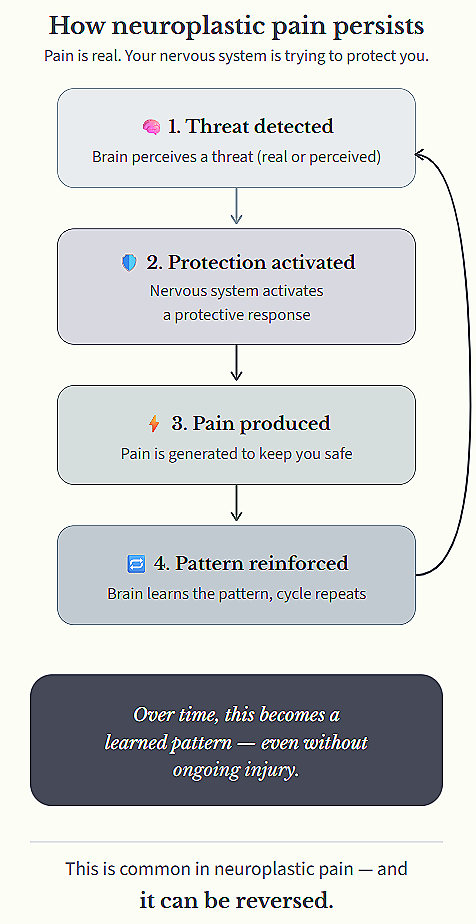
This type of pain is often called neuroplastic pain.
It is real, learned, and changeable.
This pattern is shaped by factors like:
past injury or illness
stress and emotional load
fear, attention, and expectation
meaning, context, and past experiences
None of these factors “cause” pain on their own. But together, they shape how the nervous system decides whether something is dangerous enough to hurt.
This work focuses on helping your brain update those signals—so it no longer needs to protect in the same way.
When the brain learns that it is safe again, the pattern can change—and pain often follows.
Is This The Right Approach For You?

Most people who find their way here are not new to trying to figure this out.
They’ve already explored diagnoses—back pain, migraines, fibromyalgia, pelvic pain, IBS—and may have received treatment, testing, or reassurance that “everything looks normal.”
But the symptoms continue.
What tends to matter more than the diagnosis is the pattern your symptoms follow.
This approach is often a good fit when symptoms:
have lasted longer than expected
persist despite treatment or “normal” testing
spread, fluctuate, or change over time
feel worse with stress, fear, or certain situations
When this pattern is present, symptoms are often being maintained by an overprotective nervous system rather than ongoing injury.
That means your symptoms are capable of changing— even if they’ve been present for a long time.
If you’re unsure, the FIT Criteria can help you identify whether your symptoms follow this pattern.
This work tends to be most effective for people who are:
tired of looking for a purely structural explanation
open to the idea that the nervous system may be playing a role
willing to actively engage in the process—not just try another treatment
ready to approach their symptoms in a different way
You don’t need to be fully convinced.
All you need is to be open and willing to approach your pain differently.
How Chronic Pain Therapy Works
Rather than focusing only on symptoms, this approach looks at how pain is being generated and maintained in the nervous system.
Most people I work with aren’t lacking information or effort—they’ve often tried everything. What’s missing is a way to work with the brain and body in a way that actually changes the pain response.
Pain Reprocessing Therapy (PRT)
Pain Reprocessing Therapy (PRT) helps your brain relearn that certain pain signals are not dangerous.
When the brain interprets something as a threat, it can keep pain turned on—even when there’s no ongoing injury. This isn’t imagined pain; it’s a learned pattern in the nervous system.
In sessions, we work directly with how your brain is interpreting these signals, so it can begin to dial that response back down.
Emotional Awareness & Expression Therapy (EAET)
For many people, pain is also connected to emotions that haven’t had a safe place to be processed—things like anger, grief, or internal pressure.
When these stay pushed down or unexpressed, the nervous system can stay in a state of tension or threat.
This part of the work helps bring those patterns into awareness in a way that feels safe and regulated, rather than overwhelming.
Internal Family Systems (IFS)
You may notice different “parts” of you reacting to pain in different ways—one part pushing through, another feeling overwhelmed, another trying to stay in control.
These internal dynamics aren’t problems—they’re protective. But they can also keep the nervous system activated.
This work helps you understand and shift those patterns, so your system doesn’t have to stay in that constant state of tension.
What can start to change through this work
If you’ve been living with chronic pain for a while, it can start to shape everything—how you move, how you think, how much space it takes up in your day.
This work isn’t about forcing yourself to push through or convincing yourself the pain isn’t real. It’s about changing your relationship with it in a way that actually shifts how your nervous system responds.
From constantly trying to figure it out → finally making sense of it
01
A lot of people come in feeling stuck in a loop—trying treatments, analyzing symptoms, wondering what they’re missing.
Over time, you start to see the patterns more clearly. Not just what is happening, but why.
That shift alone can take some of the urgency and pressure out of the experience—and for some people, even this begins to slightly reduce the intensity of symptoms.
From bracing against pain → feeling safer in your body
02
When pain feels unpredictable or threatening, it makes sense that your body stays on guard—monitoring, tightening, preparing.
Through this work, that constant bracing can begin to soften.
You may notice moments where your body feels a little less tense, or where the pain doesn’t escalate in the same way—or doesn’t last as long when it does.
Not because you’re ignoring it, but because your nervous system is starting to register that it’s not in danger.
From organizing your life around pain → having more room to live
03
Pain can quietly start to run the show—what you do, what you avoid, how much you push yourself, how much you hold back.
As things shift, the goal isn’t just to cope better—it’s to need to think about it less.
For many people, this includes meaningful reductions in pain over time—along with more space in your mind, more flexibility in your day, and more freedom to engage in your life again.
Frequently Asked Questions (FAQ)
-
I can’t promise that — and anyone who does isn’t being honest.
What this work offers is a way to understand why pain is happening and to create the conditions where pain can change. For many people, pain reduces significantly or resolves as the nervous system learns that it no longer needs to protect in the same way. For others, pain becomes less intense, less frequent, or less consuming.
The focus here isn’t on guarantees or quick fixes. It’s on meaningful, lasting change based on how pain actually works — not just learning to tolerate it better.
-
Sometimes — but not always.
Many people have both structural contributors and nervous system sensitization. This work can be helpful when pain:
lasts longer than expected after healing
spreads or fluctuates
feels out of proportion to current tissue findings
If pain is primarily driven by active disease, ongoing injury, or structural instability, this approach may not be appropriate on its own. Part of the work is carefully assessing whether nervous system processes appear to be meaningfully involved.
This isn’t about ignoring structure — it’s about understanding when structure alone doesn’t explain what’s happening anymore.
-
CBT and behavioral pain management tend to focus on coping with pain: pacing, thought patterns, behavior changes, and learning how to live around symptoms.
Pain reprocessing therapy (PRT) and nervous system–based approaches aim at something different. Rather than managing pain long-term, the goal is to change the pain signal itself when pain is being generated by learned threat in the nervous system.
This work is less about “thinking differently” and more about helping the brain and nervous system learn something new through experience. For people whose pain hasn’t responded to coping-based approaches, that distinction matters.
-
There isn’t a single timeline.
Some people notice shifts relatively quickly once the nervous system begins to update. Others need more time, especially if pain has been present for many years or has become intertwined with long-standing patterns of stress, fear, or self-protection.
Progress isn’t linear, and it’s not something you can force. This work is usually time-limited and purpose-driven rather than open-ended, but readiness and nervous system safety matter more than speed.
-
This work is often a good fit if:
your pain hasn’t made full sense structurally
you’ve tried many approaches without lasting change
symptoms shift with stress, attention, or context
you’re open to understanding pain differently
It may not be a good fit if you’re looking for reassurance, passive treatment, or a step-by-step formula. Curiosity, openness, and willingness to engage matter more than optimism.
If you’re unsure, that’s okay. Fit is usually clarified through careful history and conversation, not a single checklist or diagnosis.
-
This isn’t a homework-heavy approach, and it’s not about tracking everything or doing exercises perfectly.
Between sessions, the work often looks like:
noticing patterns in pain, fear, or self-protection
experimenting gently with new ways of responding to sensations
applying insights from sessions in real-life moments
The goal isn’t to work harder — it’s to support nervous system learning through lived experience, at a pace that feels sustainable rather than overwhelming.
-
I work with people experiencing a wide range of chronic pain and persistent physical symptoms, including back and joint pain, migraines, fibromyalgia, pelvic pain, tinnitus, and irritable bowel syndrome (IBS).
What matters most isn’t the diagnosis, but the pattern — particularly whether symptoms appear to be maintained by an overprotective nervous system rather than ongoing injury alone. People with very different labels can benefit from the same underlying work when those patterns are present.
-
Symptoms like Long COVID, POTS, CFS, or other chronic conditions can sometimes be maintained by an overprotective, sensitized nervous system—especially when medical testing hasn’t fully explained their persistence or severity, or when symptoms fluctuate with stress, attention, or context.
In many cases, symptoms may have been initially triggered by something real and physiological, such as a viral illness, environmental exposure, or period of significant stress. However, once the nervous system shifts into a prolonged state of threat, it can amplify symptoms and make recovery more difficult—even after the original trigger has passed or stabilized.
This work focuses on understanding whether your symptoms may be influenced by learned threat and sensitization, alongside any underlying medical factors. When that pattern is present, nervous system–based approaches can help reduce symptom intensity, reactivity, and overall impact.
That said, not all non-pain symptoms are neuroplastic, and this approach isn’t a fit for everyone. Determining whether it makes sense in your case is part of the process—and doesn’t require certainty upfront.

If this approach resonates with you, you don’t need to be certain.
You just need to be open to trying something different.
Chronic pain doesn’t usually shift by thinking about it more or trying harder.
It changes when you begin working with your nervous system in a different way—and that takes some willingness to engage in the process.
If something here felt familiar, that’s enough to take the next step.